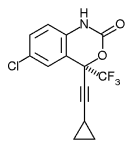
TMC125 (also spelled TMC-125, TMC 125, or etravirine), by Tibotec Pharmaceuticals Ltd., based in Cork, Ireland and now part of Johnson & Johnson, is a "second generation" NNRTI (non-nucleoside reverse transcriptase inhibitor)--an antiretroviral in the same class as efavirenz (brand name Sustiva, or Stochrin in many countries) or nevirapine (Viramune). It differs from these in being much less susceptible to viral resistance. This is not an accident; the drug molecule was carefully designed to be able to "wiggle and jiggle" so that it can change its shape in order to fit into the active pocket of the HIV enzyme reverse transcriptase and stop the enzyme from working, even when that pocket changes shape (due to resistance mutations) so that efavirenz and nevirapine will not fit. For example, the highly treatment experienced volunteers who entered the phase II trial named TMC125-C223 (reported in mid November at the 10th European AIDS Conference) had HIV that was on the average about 40 times less sensitive to efavirenz when they started the trial, and about 60 times less sensitive to nevirapine, but only 1.6 times less sensitive to TMC125.
In the 24-week data presented at the conference [1], those on combination antiretrovirals including the lower of two doses of TMC125 had a 1.04 log drop (to slightly less than 10% of the amount of virus they started with) in HIV viral load; those on the higher dose had a 1.18 log drop. These were compared with an "active control" group--volunteers who got the best regimen that could be devised for them using approved drugs. The active control had a 0.19 log drop, (not statistically significant). This group did show a modest improvement earlier in the 24 weeks, as much as half a log, probably because of the switch to a regimen carefully designed for them at that point in time.
The size of the viral load drop from TMC125 depended very much on having other active drugs in the regimen. Those with no other active drug (because they were resistant to all the other drugs in their regimen) averaged only about a half-log drop (average of the two TMC125 doses). Those whose virus was sensitive to one antiretroviral in addition to TMC125 had an average one-log drop or a little less; those sensitive to two other antiretrovirals averaged about one and a half logs HIV reduction, or a little more.
Note: As this article went to press we learned that one phase II trial, TMC125-C227, is being stopped early. This trial tested TMC125 in volunteers who had received an NNRTI (usually efavirenz or nevirapine) and had at least one resistance mutation to it. The trial was stopped because some of these volunteers had a poor antiviral response to TMC125; those in the control group, who were treated with protease inhibitors instead, did better in reducing viral load. The new phase III trials--which use a different formulation of TMC125 with a different group of patients--have not been changed. The C227 trial was being conducted in eight countries, not including the U.S. We will be watching for more information on what happened in this discontinued trial.
Two Phase III Trials Starting
On November 17, 2005 Tibotec announced the start of two phase III "pivotal" trials with 600 heavily treatment experienced patients each, to be conducted in 18 countries. These trials are unusual in combining two experimental drugs. TMC125 will be combined with TMC114, a new protease inhibitor also from Tibotec. These similar trials are called DUET 1 (official name TMC125-C206) and DUET 2 (TMC125-C216).
For more information about these (or other) clinical trials in the U.S, see http://www.clinicaltrials.gov; search for "TMC125" (quotation marks not necessary).
References
(1.) Nadler JP, Grossman HA, Hicks C, and others. Efficacy and tolerability of TMC125 in HIV patients with NNRTI and PI resistance at 24 weeks: TMC125-C223. 10th European AIDS Conference/EACS, November 17-20, 2005, Dublin, Ireland [abstract LBPS3/7].
COPYRIGHT 2005 John S. James
COPYRIGHT 2005 Gale Group




 Home
Home A
A E-Base
E-Base