The 200 mg capsules of efavirenz are gold-colored, reverse-printed with "SUSTIVA" on the body and imprinted with "200 mg" on the cap. Other dose formulations are available.
"Dupont Pharma has engaged in opportunistic pricing and dramatically increased the cost threshold for drugs of this type."
--Martin Delaney of Project Inform
"The individuals who lead the Fair Price Working Group, as well as the individuals and organizations that are signatories to its consensus statement on the pricing of efavirenz, represent some of the most prominent and respected precincts of AIDS advocacy. Ninety-one organizations and 165 individuals have signed on to the Group's effort. Although we respect their collective judgment and commitment, we take issue with their reasoning and dissent from their conclusions."
--Paul Simmons, RN, ACRN, for the staff of The Center for AIDS
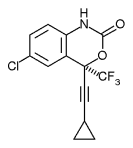
Also known as: EFV, DMP-266
Background and description. Efavirenz is a non-nucleoside reverse transcriptase inhibitor (NNRTI) manufactured by DuPont Pharmaceuticals Company. The drug was granted approval by the US Food & Drug Administration (FDA) in September 1998 to treat HIV infection.
Guidelines classification. The Panel on Clinical Practices for the Treatment of HIV Infection classifies efavirenz as a "strongly recommended" NNRTI.
Dose. The recommended dose of efavirenz is 600 mg (three 200 mg capsules)once a day.
Food restrictions. Efavirenz may be taken with or without food. However, a high fat meal may increase the absorption of efavirenz and should be avoided.
Storage. Capsules should be stored at 77 [degrees] F. Short-term temperature variations from 59 [degrees] to 86 [degrees] F are acceptable.
Side effects and toxicity. The most common side effects of efavirenz are related to the central nervous system. In clinical trials side effects included dizziness, sleep disturbances, nightmares, hallucinations and confusion. These side effects occurred in over 50% of patients with a median duration of 21 days. Serious depression has been seen in a small number of patients, as well as treatment-related psychosis. In addition, rash has been reported in approximately 30% of patients. Most rash resolves when drug is discontinued and does not recur upon resumption. More severe cases of rash have been known to appear in children. Other side effects include nausea and diarrhea, as well as elevated lipid levels, especially when efavirenz is combined with protease inhibitors.
Drug interactions. Efavirenz should not be taken with the following: midazolam (Versed), triazolam (Halcion), cisapride (Propulsid) and ergot derivatives (Wigraine and Cafergot). Levels of clarithromycin (Biaxin) and rifampin (Rifadin, Rimactane) are reduced by efavirenz. The significance of such reduction is unknown. Levels of rifabutin (Mycobutin) are also reduced by efavirenz and an increase in dose of rifabutin to 450 mg should be considered.
Efavirenz should not be combined with saquinavir (Fortovase, Invirase) since such co-administration significantly decreases the levels of saquinavir. Indinavir (Crixivan) levels are reduced by efavirenz and an increase of indinavir to 1000 mg every 8 hours should be considered. Amprenavir (Agenerase) and efavirenz should not be combined without the addition of 200 mg of ritonavir (Norvir) or the addition of a full dose of nelfinavir (Viracept). Efavirenz lowers the levels of lopinavir (also known as ABT-378), Abbott Laboratories' soon-to-be-approved protease inhibitor. A dose increase in lopinavir may be necessary for protease experienced patients but not for protease naive patients when combining lopinavir with efavirenz.
Resistance and cross-resistance. A mutation at position 103 confers resistance to efavirenz and results in virologic failure. Other common mutations occur at positions 100, 108, 179, 181 and 188.
Clinical data. Approval of efavirenz was based on 2 clinical trials in which the response was measured as time to treatment failure. Study 006 is an ongoing, randomized, open-label trial comparing efavirenz/ indinavir (Crixivan) against efavirenz/zidovudine (Retrovir)/lamivudine (Epivir) against indinavir/ zidovudine/lamivudine. At 48 weeks the percentage of patients with viral loads below 50 copies/mL was 68% for the efavirenz/zidovudine/lamivudine group compared to 55% for the efavirenz/indinavir group and 49% for the indinavir/zidovudine/lamivudine group. The overall mean increase in CD4 T cells across arms was 200 cells/[mm.sup.3].
ACTG 364 is a randomized, double-blind, placebo-controlled study in nucleoside reverse transcriptase inhibitor (NRTI) experienced patients. Patients received efavirenz/NRTIs or nelfinavir/NRTIs or efavirenz/nelfinavir/NRTIs. The overall mean increase in CD4 T cell count was approximately 100 cells/mm3 at 48 weeks among patients who continued their regimens. The percentages of patients with viral loads below 500 copies/mL were as follows: 71% for the efavirenz/nelfinavir/NRTIs arm; 60% for the efavirenz/NRTIs arm; and 33% for the nelfinavir/ NRTIs arm. Additional studies have shown that efavirenz may successfully achieve and maintain viral suppression without a protease inhibitor, thus sparing protease inhibitors as a class available for subsequent therapy.
Patient assistance. Patients can contact the Efavirenz Reimbursement Counseling & Assistance Program at 800.334.4486.
COPYRIGHT 2000 The Center for AIDS: Hope & Remembrance Project
COPYRIGHT 2000 Gale Group




 Home
Home A
A Growth hormone
Growth hormone